
Women should be offered a full range of non-surgical options before having vaginal mesh surgery, new draft guidelines from the National Institute for Health and Care Excellence (NICE) state.
The guidelines, for the treatment of stress urinary incontinence (SUI) or pelvic organ prolapse, come in the wake of the vaginal mesh scandal, where hundreds of thousands of women worldwide reported life-changing complications after surgery, such as extreme pain and being unable to walk.
The guidelines also recommend the suspension on vaginal mesh surgery announced by the government in July continues until a set of criteria are met. These include registering all operations and any complications on a national database and ensuring surgery is being performed by specialist surgeons based at specialist centres.
But Kath Sansom, founder of campaign group Sling The Mesh, told HuffPost UK the guidelines “do not go far enough”.
“Our ideal scenario is to see pelvic mesh stopped. Full stop. The risks are too great. It is totally unacceptable that women come out of a ‘simple little operation’ with shattered lives,” she said.
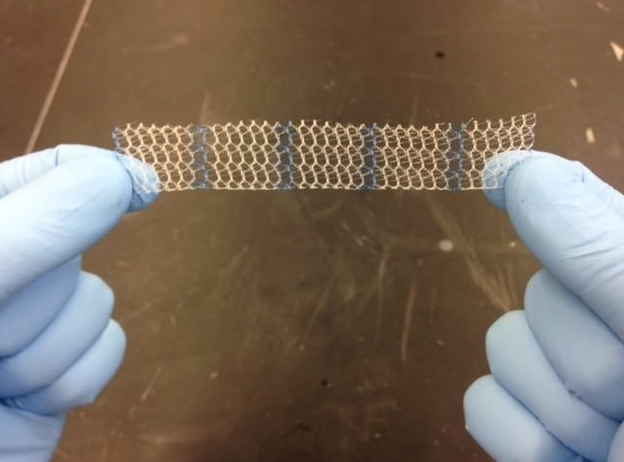
[READ MORE: What is vaginal mesh?]

Vaginal mesh, sometimes referred to as a “sling” or “tape”, is a synthetic material implant inserted into the body to join weakened tissue. It’s used to treat both pelvic organ prolapse and urinary incontinence, which can affect women after childbirth.
There are a number of non-surgical options for both urinary incontinence and pelvic organ prolapse detailed in the report, which NICE says should be considered before surgery.
The non-surgical options for urinary incontinence include:
- Lifestyle interventions (such as moderating caffeine intake and losing weight)
- Physical therapies (such as pelvic floor muscle training)
- Behavioural therapies (such as bladder training programmes)
- Medicines
Non-surgical options for pelvic organ prolapse include:
- Lifestyle modification (such as losing weight, avoiding heavy lifting)
- Topical oestrogen
- Pelvic floor muscle training
- Pessary management
Surgical interventions using surgical mesh should only be considered when non-surgical options have failed or are not possible, the report states.
In a statement given to HuffPost UK, chair of the All-Party Parliamentary Group on Surgical Mesh Implants, Owen Smith MP, said: “This is a welcome U-turn from NICE, who in their 2016 guidelines for mesh did not recommend any other treatment options for SUI and in fact stated that complications from mesh were ‘infrequent’.
“While I am pleased that NICE is now taking action to advise against mesh as a first-line treatment, this announcement is well overdue. I have called on them to get on and urgently publish these guidelines for the last two years and I’m glad they have finally listened. This news is also a complete vindication of the thousands of women injured by mesh surgery who have campaigned tirelessly to get the procedure halted.”
The NICE report also reiterates a national database should be set up to record all procedures involving the use of surgical mesh in operations for stress urinary incontinence or pelvic organ prolapse, to help with future decision making.
In recent months women around the world have claimed they were unaware of potential risks of vaginal mesh surgery before undergoing their operations.
Cat Lee, a former Huddersfield University lecturer, who had to give up her job due to complications, said she initially jumped at the chance to have the surgery.
“Ten years on, I’m convinced that the so-called ‘simple’ vaginal mesh surgery has ruined my life,” the mum-of-two said. “I can only do the school run a few times a week and then, he [Cat’s youngest son, Charlie] has to walk alongside me in my mobility scooter. I can’t play with him like other mums and I don’t feel like much of a wife either.”
The new guidelines state that in the cases where it is agreed to use surgical mesh, women must be fully informed of the risks. A follow up appointment should be offered within six months to all women who have had urinary incontinence or prolapse surgery and any complications should be assessed and managed by consultants working at centres specialising on the issues.
Complications related to the device should be reported to the Medicines and Healthcare products Regulatory Agency (MHRA) and details of the complications should be collected in a national registry.
Kath Sansom, founder of Sling The Mesh, told HuffPost UK: “These draft guidelines are to be welcomed but they do not go far enough.”
“NICE recommend mesh implants should only be used as second line treatment, but we want to make it the third line treatment option, to ensure only the smallest number of women are exposed to mesh risk,” she said.
“NICE say mesh can be offered after conservative treatments like physiotherapy or pessaries fail. But we say it should only be offered after both conservative treatments fail and after non-mesh surgeries fail. That way it is a belt and braces approach so that mesh truly is the last resort.”
A survey of Sling the Mesh members found one in seven have lost their marriages because of mesh and one in seven have lost their sex life. Eight out of 10 suffer pain so great it affects their daily life and more than half suffer ongoing urinary infections. Some members expressed suicidal thoughts and six in 10 are on anti depressants.
“Although we are delighted that finally NICE recognises the grave and serious complications, sadly many thousands of women have been harmed in the last 20 years,” Sansom added. “This guidance should have come a long time ago.”